POST-EXTRACTION PROTOCOL
BASICS, per Martin Fischer, MD
Excerpts from
Martin Fischer, Death and
Dentistry, 1940, pertaining to post-extraction protocol, as compiled by S.H. Shakman,
InstituteOfScience.com)*:
80
The x-ray
helps in diagnosis only when bone absorption is prominent;
sometimes when additional calcium has been deposited. Positive
roentgenograms of the situation are therefore few.
118
Figure 43, which
faces p. 87, shows how little is the amount of cancellated as
opposed to petrous bone to be seen about an adult molar in the
lower mandible. When
now it is recalled that the already meager blood supply to those
petrous portions arrives via the cancelleted, it becomes
apparent why even slight injury thereto threatens the life of
all jaw substance distal to a root tip. In the clinical
instance then, matters are usually worse. 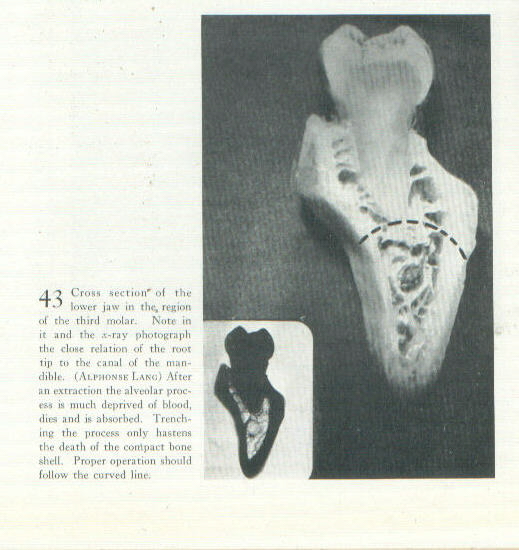
120
“What is at
stake was perfectly clear to John Hunter though we have not had
the sense to apply his teachings these one hundred and fifty
years. Said he:
‘The Alveolar Processes of both Jaws should rather be
considered as belonging to the Teeth, than as parts of the
Jaws; for they begin to be formed with the Teeth, keep
pace with them in their growth, and decay, and entirely
disappear, when the Teeth fall … In short, there is such mutual
dependence of the Teeth and Alveolar Processes on each other,
that the destruction of the one seems to always be attended with
that of the other.”
… “We
do not always dress to the ultimate resorption line at once,
simply because the alveolar bone is infected and line of
demarcation of infection is ‘vague.’ … So for a month or
two after an extraction we incline to let the patient rest, in
order better to know how much [121] of what remains of
peridental bone assumes healthy form. Then the still
affected alveolar process, now more definitely demarcated,
is attacked a second time. …”
“… Every still
reddened gum points to an area of infection beneath; and if the
gum appears normal, every spot sensitive to finger ball
pressure. Nothing is worse for the patient than the assumption
that an infection of the alveolar processes has been set aside
“because the x-ray is negative.”
136
“Infected
residual bone requires removal! Toward this end, how
far may and must the operator go?
The answer is, at least to the level of the ‘true’
bone constituting the maxillae proper. And in making
such attack, what should be the design of his operation? Commonly the dentist
‘trenches’ the lower or upper jaw, meaning that he removes first
the cancellated portions of these structures to leave the
petrous walls standing. He
should, on the contrary, remove these petrous portions
(including the interdental) first, rounding off the medullary
portion, as it were.
The situation is portrayed diagrammatically in Fig 43
facing p 87. There
is no purpose even in saving reflected periosteum – it is
better destroyed, for when saved, any ‘regeneration’ of bone
that is likely to appear from it is of exostotic variety,
probably infected and at all times useless. Its salvation has in
our experience only proved earlier notice that another
operation for removal of bone would be required.
* For further
information on the need to remove alveolar bone following
extraction, please see Death
and Dentistry, 1940, by Martin Fischer MD, particularly
pages: 52-3, 56, 61, 64, 77, 80, 86-7, 112, 116-120, 135-7, 140,
146-8, 152, 161-3, 171, 173, 180-6.
